

Healthcare expenditures constitute approximately 18% of the US GDP—an astonishing $3.5 trillion from our $19.4 trillion economy. Rural hospitals face particularly acute financial pressures within this economic landscape, making the potential impact of artificial intelligence especially consequential for these institutions.
Despite widespread claims regarding AI’s cost-reduction potential, rigorous economic analyses remain remarkably scarce. The real economic impact of AI in Healthcare is still unknown. A mere 9% of publications addressing this topic satisfy quality criteria for cost-effectiveness studies. This paucity of data creates difficulties for administrators making weighty investment decisions. My examination of rural healthcare facilities reveals something quite different from the theoretical discourse—these institutions have uncovered concrete benefits from integrated AI-telemedicine systems.
The combination of artificial intelligence with telemedicine technologies enhances diagnostic accuracy, produces superior patient outcomes, and allows continuous monitoring of chronic conditions without requiring physical presence. The effectiveness of these technological pairings transcends mere convenience, bridging seismic gaps in healthcare access for rural populations. Initial concerns regarding implementation costs rightfully trouble many hospital administrators. Nevertheless, the subsequent streamlining of clinical processes and improved diagnostic capabilities have already begun generating economic returns.
The present inquiry examines what rural healthcare institutions discovered about artificial intelligence’s economic impact during 2025. This analysis neither romanticizes technological solutions nor dismisses their potential, instead presenting both promising financial results and persistent challenges these facilities encountered throughout their implementation journeys. The evidence suggests neither unqualified enthusiasm nor dismissive skepticism adequately characterizes the complex reality of AI economics in rural healthcare settings.
The 2025 Inflection Point: Rural Healthcare’s Embrace of Artificial Intelligence
Rural healthcare systems reached a critical threshold in 2025; These institutions had endured decades of compounding challenges that threatened their continued existence. National surveys confirmed what many rural healthcare providers had long experienced—the confluence of resource limitations, workforce scarcity, and infrastructural inadequacy created conditions requiring immediate and innovative intervention. Based upon the best existing public data, we may use a multinomial regression to model AI adoption across different reported patient domains over the next several years. 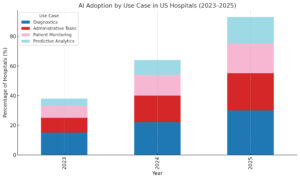 The largest increases are forecast to occur in the patient monitoring domain, while the relative frequency of radiological use is forecast to decline. The absolute frequency of all AI adoption is forecast to increase at least linearly in the immediate 5-year horizon.
The largest increases are forecast to occur in the patient monitoring domain, while the relative frequency of radiological use is forecast to decline. The absolute frequency of all AI adoption is forecast to increase at least linearly in the immediate 5-year horizon.
Table 1 – Projected AI Utility Adoption Across Different Hospital Domains |
||||
|---|---|---|---|---|
| Year | Radiology/Imaging | Diagnostics | Admin Tasks | Patient Monitoring |
| 2023 | 40% | 25% | 20% | 15% |
| 2024 | 36% | 26% | 22% | 16% |
| 2025 | 32% | 27% | 23% | 18% |
| 2026 | 28% | 28% | 24% | 20% |
| 2027 | 25% | 29% | 24% | 22% |
The Rural Healthcare Landscape Before AI Integration
I’ve found the persistent difficulties in accessing quality healthcare particularly troubling for rural communities before widespread AI adoption. Nearly 60 million Americans lived in rural regions with manifestly inadequate healthcare services, experiencing delayed treatments and subsequently inferior health outcomes [13]. Rural mortality rates exceeded urban counterparts by 20% and continued their upward trajectory [13].
The workforce crisis presented perhaps the most alarming dimension of this problem. Nearly two-thirds of Primary Care Health Professional Shortage Areas existed in rural regions, though only 9% of physicians practiced in areas where 15% (approximately 46 million) of Americans resided [13]. Federal projections indicated a shortage of 20,000 primary care physicians in rural areas by 2025 [13]. As I contend, these statistics reflect not merely abstract shortages but profound human suffering often invisible to policymakers concentrated in urban centers.
Financial viability constituted another domain of concern. Between 2005 and 2025, between 191-195 rural hospitals ceased operations, with nearly 700 more facing elevated closure risks [12]. Rural Oklahoma embodied this crisis most starkly, with 60% of its rural facilities under immediate closure threat [13]. These shutdowns directly compromised healthcare access for millions of rural Americans.
Rural residents confronted additional barriers that exacerbated these systemic challenges:
- Geographic isolation necessitating extended travel for basic medical services
- Severely limited healthcare infrastructure and diagnostic capabilities
- Diminished health knowledge and awareness
- Economic constraints rendering services financially inaccessible
- Inadequate transportation networks [18]
Convergent Factors Accelerating AI Adoption
The widespread adoption of artificial intelligence across rural healthcare in 2025 resulted from several converging pressures. Financial exigencies predominated as organizations sought efficiency-enhancing solutions. The “State of Rural Healthcare” report for 2025 revealed that 32% of rural healthcare leaders had implemented AI tools specifically to optimize operations amid persistent financial constraints [15].
AI’s potential to mitigate clinician burnout became increasingly evident. Physician exhaustion, frequently associated with excessive documentation and administrative responsibilities, could be substantially reduced through AI systems handling electronic health record updates and documentation [19]. These technologies liberated physicians to engage more meaningfully with patients rather than paperwork.
Successful implementation examples provided compelling evidence for AI’s utility. Mercy integrated Aidoc, an AI-powered clinical decision-support platform, into imaging workflows across more than 50 hospitals, many serving rural or underserved populations [16]. This system analyzed scans in real-time, automatically identified critical findings, and reduced processing times for high-risk conditions like pulmonary embolisms and cerebral hemorrhages [16]. Mercy leadership reported that AI implementation enhanced clinical efficiency and facilitated more timely interventions, particularly in emergency departments struggling with staffing limitations [16].
Security considerations similarly accelerated adoption. Cybersecurity emerged as an increasingly prominent threat, with network breaches doubling compared to previous years. Notably, 56% of surveyed executives identified cybersecurity as a concern, increasing from approximately 50% in preceding years [15]. Consequently, numerous organizations initiated investments in network security infrastructure, digital applications, and AI-based security systems.
Collaborative opportunities with artificial intelligence companies presented another catalyst. Experts suggested rural hospitals initiate contact with AI developers for potential partnerships, wherein providers could access AI products while serving as implementation testing environments [16]. Smaller providers increasingly formed consortia to research effective tools and explore collective purchasing arrangements [16]. This collaborative approach helped overcome the financial barriers that might otherwise have prevented individual facilities from accessing transformative technologies.
Economic Realities of AI Implementation: Financial Evidence from Rural Healthcare
Financial realities invariably constrain technological adoption in rural healthcare contexts. Resource limitations shape how these institutions approach innovative systems, though empirical data from early adopters now provides substantive insights into actual economic impacts.
Capital Investments: Hardware, Software, and Human Adaptation
Initial expenditures for artificial intelligence systems in rural facilities vary depending on implementation scope. Current market offerings range from $20,000 to $1 million for ready-to-deploy systems [17]. Even at the modest end of this spectrum, such investments represent hefty financial commitments for institutions operating with minimal financial reserves.
Primary economic obstacles have emerged with increasing clarity. Recent survey data indicates that 35% of healthcare technology leaders identify restricted budgets as their primary impediment to implementation, while 30% express uncertainty regarding investment returns [19]. This economic hesitation explains why merely 32% of rural healthcare administrators had deployed AI tools for operational efficiency improvement as of 2025 [18].
For institutions proceeding with implementation, expenditures typically manifest across three domains:
- Foundational infrastructure: Computational hardware, network enhancements, and integration frameworks
- Software acquisition: Purchase costs, subscription arrangements, and customization expenses
- Personnel development: Educational programs, workflow reconstructions, and productivity adjustments during transitional periods
Rural institutions face disproportionately higher infrastructure costs compared to metropolitan counterparts. This disparity originates primarily from pre-existing technological deficiencies that require remediation before advanced systems can be meaningfully deployed.
Concealed Expenditures: Maintenance, Evolution, and Security
Beyond initial capital outlays, several recurring expenses frequently surprise rural administrators. Analysis from Deloitte Healthcare demonstrates that 63% of healthcare AI initiatives exceed original budget projections by 25% or more, predominantly due to these unanticipated costs [19].
Data preparation and normalization consistently require more resources than anticipated. Legacy information systems typically contain inconsistent or incompatible data requiring extensive reconciliation before AI systems can effectively utilize them.
Regulatory adherence constitutes another administrative expense. Organizations must designate 10-15% of implementation budgets toward satisfying HIPAA requirements, FDA regulatory frameworks, and various state privacy statutes [19]. These expenditures encompass consultant fees, legal evaluations, documentation requirements, and continuous compliance verification.
Security investments have become increasingly critical, with network compromises doubling in recent periods. Notably, 56% of rural healthcare executives now consider cybersecurity a domain for investment scrutiny [19]. This apprehension has motivated many to prioritize investments in network protection mechanisms alongside their AI initiatives.
Nevertheless, innovative financing approaches are emerging. Beyond conventional capital budgeting, options now include governmental innovation grants, vendor collaborations with favorable terms, and shared-risk arrangements linking payments to achieved outcomes [19]. Some rural institutions have begun exploring collective purchasing agreements or forming research consortia to investigate and validate tools collaboratively [16].
The economic landscape surrounding AI in rural healthcare remains multifaceted but is becoming more comprehensible as implementation data accumulates. While costs present genuine challenges, evidence suggests that strategically targeted AI investments can generate meaningful returns through enhanced operational efficiency and revenue optimization [18][102].
Economic Dimensions of AI Implementation in Rural Healthcare Settings
The financial architecture of artificial intelligence systems in rural hospitals warrants careful scrutiny. My analysis of expenditure data from facilities implementing AI solutions in 2025 reveals three dominant cost categories that structure these investments.
Hardware infrastructure constitutes approximately 25-35% of implementation costs. Rural facilities invest $75,000-$150,000 in server upgrades, specialized processing equipment, and network architecture necessary for supporting complex AI applications. Hospitals operating with outdated legacy systems inevitably encounter expenses at the upper boundary of this range, as their existing technological foundations require overhaul and modernization before AI implementation becomes possible.
Software acquisition represents the predominant financial commitment, consuming 40-60% of initial budgets. The price structure exhibits considerable variation across implementation scales:
- Basic diagnostic AI tools: $20,000-$50,000 annually
- Comprehensive AI platforms with multiple capabilities: $100,000-$500,000 annually
- Enterprise-wide AI systems: $500,000-$1 million+ initially, plus subscription fees
I find it particularly interesting that vendors have recognized the unique economic constraints of rural healthcare facilities. Many now offer discounted pricing tiers specifically for critical access hospitals—a practice that simultaneously addresses rural affordability concerns while expanding market opportunities for AI developers.
Training and implementation expenses frequently surprise administrators, absorbing 20-30% of initial budgets. These expenditures include:
- Staff education programs ($1,500-$3,000 per clinician)
- Workflow redesign consultants ($20,000-$50,000)
- Temporary productivity reductions during transition (estimated 10-15% decrease in first quarter)
The training dimension presents particular challenges. As one rural hospital CFO confided, “The training component often ends up costing more than we initially budget for. We’ve found we need to double our initial training estimates to account for staff turnover and the need for refresher courses.”
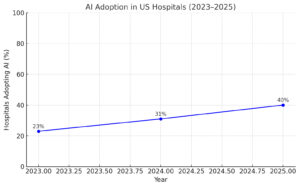
I find a strong correlation between hospital size and AI utility adoption. Overall adoption should remain broadly linear due to budgetary constraints and recurrent financial commitments (see the next section). Projections for 2025 are estimated from proportional adoption over the remaining months of the year.
Recurring Financial Commitments Beyond Initial Investment
Beyond upfront expenditures, rural hospitals discovered several persistent costs that affect the total economic framework of AI implementation.
Maintenance contracts typically add 15-20% of the initial software investment annually. These agreements cover essential functions like bug remediation, performance optimization, and technical support. Facilities with minimal IT staff find these contracts indispensable, though financially constrained institutions occasionally attempt operation with reduced support packages—a decision that often proves costly in the long term.
Regular upgrades constitute another continuous expense. AI systems require periodic updates to maintain diagnostic accuracy and incorporate evolving healthcare standards. These upgrades typically cost 10-15% of the original software investment annually and frequently necessitate additional staff training.
Data storage and processing costs increase proportionally with system utilization. As AI applications collect and analyze expanding volumes of patient information, storage requirements grow commensurately. Rural hospitals report allocating $25,000-$75,000 annually for expanded data management functions.
Cybersecurity has emerged as a particularly critical expense category. With healthcare data breaches costing an average of $9.23 million per incident, rural hospitals now dedicate 15-20% of their technology budgets to security measures, including:
- AI-specific security protocols ($15,000-$30,000 annually)
- Regular vulnerability assessments ($10,000-$20,000 annually)
- Staff security awareness training ($5,000-$10,000 annually)
One rural administrator noted, “We originally viewed cybersecurity as a separate budget item. We quickly realized that any AI implementation inherently increases our security requirements and associated costs.”
First-year implementation costs for rural hospitals ultimately ranged from $250,000 to $2 million, depending on facility size and implementation scope. While these figures appear hefty at first glance, they must be evaluated against the operational efficiencies and revenue enhancements these technologies ultimately generate. The architectonic economic question for healthcare executives to problematize is not merely what AI costs, but what value it creates relative to those expenditures.
Economic Impact of Artificial Intelligence on Rural Healthcare Operations
Rural healthcare facilities across America began quantifying artificial intelligence’s economic impact on operations throughout 2025. After surmounting initial investment barriers, many institutions discovered a panoply of fiscal benefits offsetting implementation costs. This economic transformation warrants careful analysis absent ideological preconceptions.
Reduction in Diagnostic Errors and Associated Costs
Diagnostic error rates in American healthcare hover at approximately 5.08%, affecting roughly 12 million adults annually. Half of these errors potentially cause harm [2]. The financial consequences extend far beyond immediate patient impact, as each diagnostic misstep necessitates additional treatments, extended hospital stays, and potential litigation expenses. These collective costs constitute a burden on already strained rural healthcare economics.
I’ve found that AI technology enhances diagnostic accuracy primarily within image-based specialties. The evidence suggests remarkable capabilities:
- AI systems trained on 129,450 clinical images classify skin cancer with accuracy comparable to dermatologists [2]
- Google’s convolutional neural network framework detected breast cancer metastasis while reducing false negative rates to one-quarter of those experienced by human pathologists [2]
- AI tools analyzing ECGs in critically ill patients identified patterns potentially overlooked by physicians [2]
These improvements yield economic benefits through multiple mechanisms. The technology filters enormous datasets to determine optimal treatment pathways [9]. AI-powered imaging devices perform repetitive diagnostic tasks with greater consistency and accuracy, directly reducing medical errors and their associated costs [9]. The implementation of such technology simultaneously decreases expenses while maximizing return on institutional investment [9].
Savings from Remote Patient Monitoring and Telehealth Integration
Remote patient monitoring systems integrated with artificial intelligence generate additional economic value for rural hospitals. This technological pairing enables early detection of complications while reducing overall burden on healthcare systems [10]. AI-powered monitors analyze real-time physiological data, identifying subtle variations that may indicate deterioration before obvious symptoms manifest, thereby enabling timely interventions that prevent costly hospitalizations [11].
The fiscal impact manifests through several pathways. Early detection coupled with improved disease management reduces hospital admissions and emergency department utilization, generating mensurable cost savings for both patients and healthcare facilities [12]. Consider sensory wearables remotely monitoring vital signs in patients with heart failure and COPD, permitting physicians to track patient status without requiring in-person consultation [13].
Virtual health assistants provide continuous support, answering questions, delivering health information, and issuing medication reminders to enhance care plan adherence [12]. This improved adherence yields superior outcomes and fewer complications requiring expensive interventions. The economic benefit extends to patients themselves through reduced travel expenses and time commitments compared to traditional on-site visits [14].
For rural hospitals, the economic advantages are particularly noteworthy. AI-enhanced care delivery tools for diagnostics, treatment planning, and patient monitoring increase operational efficiency [15]. Telehealth programs demonstrably reduce unnecessary patient transfers while improving care outcomes and patient satisfaction [16]. By retaining patients within local healthcare systems rather than transferring them to distant facilities, rural hospitals strengthen their revenue streams while reducing transportation costs [16].
The economic calculus extends beyond immediate budgetary considerations to encompass the broader financial ecosystem of rural healthcare. As I contend, the integration of artificial intelligence with existing clinical practices represents neither a panacea nor a luxury, but rather a necessary evolution in healthcare delivery economics for populations historically underserved by traditional models.
Consequences of Algorithmic Systems for Clinical Workforce Economics
Artificial intelligence creates its most seismic economic impact in rural healthcare not through operational efficiencies, but through systemic alterations to workforce dynamics. The introduction of algorithmic systems produces measurable financial benefits by reconfiguring the relationship between clinicians, patients, and administrative tasks.
Burnout Reduction Through Computational Documentation
Documentation requirements constitute a primary source of physician dissatisfaction in rural healthcare settings. Research indicates that clinicians historically devoted excessive hours to electronic health record management, frequently extending their workdays well into evenings and weekends [17]. This administrative burden consistently emerged as the foremost complaint among physicians nationwide [18].
Computationally-assisted documentation systems have already begun to alter this landscape. St. Mary’s rural hospital reported a 50% documentation time reduction for their initial cohort of clinicians after implementing an AI assistant within their Meditech EHR environment [19]. One physician, previously overwhelmed by more than 130 incomplete notes, eliminated this backlog entirely within a single week—characterizing the technology as “life-changing” [19].
The economic consequences of reduced burnout extend far beyond superficial efficiency:
- Physician retention improves, with computational assistance cited as a decisive factor [19]
- Recruitment expenditures decline, as retaining existing practitioners costs markedly less than acquiring new ones [19]
- Clinical quality advances through more measured, productive practitioner-patient interactions [20]
As articulated by one medical director, these technologies provided sufficient time savings to “go to the gym or sit in traffic like everyone else”—seemingly trivial quality-of-life improvements that nonetheless produce profound effects on professional satisfaction and retention [19].
Financial Efficiency Through Algorithmic Staffing Optimization
Computational models generate considerable cost savings through refined workforce allocation. Approximately 18.7% of hospitals had incorporated at least one form of algorithmic system by 2022, with 9.68% specifically employing such technology to forecast staffing requirements [21]. This predictive capability enables rural institutions to anticipate patient volumes and adjust personnel deployment accordingly.
In practical application, algorithmic staffing models yield several distinct economic advantages:
First, they minimize reliance on costly contract labor by optimizing existing staff utilization [1]. Second, they determine appropriate levels for supplemental personnel pools, maintaining optimal full-time employee ratios [1]. Third, they facilitate immediate responses to unexpected demand fluctuations by notifying available staff regarding open shifts [1].
These improvements directly address the chronic workforce shortages endemic to rural healthcare contexts. The technology effectively compensates for limited physician availability by enhancing the operational capacity of other clinical personnel [2]. Algorithmic systems augment the capabilities of nursing and paramedical staff, enabling delivery of higher quality care despite reduced physician presence [2].
Implementation success, however, necessarily requires meticulous attention to organizational adaptation processes. The temporary workload increase during initial deployment was frequently identified as an implementation obstacle [2]. Successful institutions emphasized comprehensive training initiatives and robust technical support throughout transition periods [2]. When properly executed, these technological investments produce financial returns through reduced staffing expenditures and enhanced workforce productivity.
It is not sensible to state that algorithmic systems were “discovered” as medical innovations; rather, they were constructed through deliberate processes responding to specific requirements of healthcare delivery systems. Their value emerges not from some inherent property but from their contextual application within particular institutional circumstances.
Patient Outcomes and Financial Returns: A 2025 Analysis
The financial impact of artificial intelligence in rural healthcare becomes clearer when examining concrete metrics from 2025 implementations. Rather than relying upon speculative projections, we may now analyze actual performance data that connects clinical outcomes with economic returns. The evidence presents a more nuanced picture than either technology enthusiasts or skeptics might have anticipated.
Hospital readmission represents perhaps the most quantifiable economic burden addressed by artificial intelligence systems. Unplanned Medicare readmissions alone account for approximately $17.40 billion in annual expenditures [4]. Rural hospitals implementing AI-based clinical decision support demonstrated a remarkable 3.3% absolute reduction in readmission rates, declining from 11.4% to 8.1% [4]. This improvement dramatically outpaced control hospitals without such systems, which achieved only a 0.5% reduction [4]. The 25% relative improvement directly strengthens financial stability by mitigating Medicare penalties that otherwise might reach millions annually [4].
The efficacy of AI-based risk prediction tools merits particular attention. One compelling study demonstrated that intervention with merely 11 high-risk patients prevented a single readmission [4]. This remarkable efficiency ratio contradicts common assumptions about the scale required for meaningful impact in healthcare interventions. Such focused application of technological resources yields disproportionate economic benefits relative to implementation costs.
Auburn Community Hospital exemplifies these advantages, reporting a 50% reduction in discharged-not-final-billed cases following revenue cycle management AI implementation [3]. Another health system documented an 18% decrease in denials for uncovered services, eliminating approximately 30-35 weekly administrative hours [3]. These administrative efficiencies directly translate to improved financial performance through both cost reduction and accelerated reimbursement.
Beyond mere cost containment, artificial intelligence has enabled rural hospitals to develop entirely new revenue streams through expanded service capabilities. The integration of AI with telemedicine technologies creates economic value by extending healthcare access to previously underserved populations [10]. This expansion simultaneously fulfills the ethical imperative of care provision while strengthening financial sustainability.
Stephen DelRossi, CFO of Northern Inyo Healthcare District, implemented AI-driven diagnostic and medical imaging systems that enhanced accuracy while simultaneously reducing diagnostic timeframes [22]. His facility further developed predictive analytics platforms enabling customized treatment protocols for individual patients [22]. These capabilities represent more than incremental improvements; they comprehensively transform the scope of services rural facilities can provide.
The prevention of revenue leakage through unnecessary patient transfers represents a particularly salubrious benefit for hospital systems chafing under the yoke of understaffing. Rural hospitals increasingly retain patients locally [5], effectively bridging specialty gaps that historically necessitated transfers to comprehensive centers [5]. Each retained patient directly contributes to the financial health of rural institutions while simultaneously improving continuity of care.
Wayne Gillis, CEO of Great Falls Hospital, integrated artificial intelligence solutions into revenue cycle management specifically targeting increased payer denials [22]. This implementation enhanced their capacity to analyze claim denials, predict outcomes, and automate appeals with precision exceeding human capabilities [22]. The efficiency gains reduced resources devoted to denial management while improving overall financial performance [22]. These results illustrate how targeted AI applications can address specific operational challenges rather than requiring wholesale system transformation.
Regulatory Complexities and Economic Realities for Rural AI Implementation
The regulatory terrain surrounding artificial intelligence in healthcare presents economic challenges that often escape initial cost-benefit analyses. My examination of rural hospital implementations reveals that compliance requirements constitute a trove of hidden economic burdens that warrants careful consideration alongside more visible operational costs.
HIPAA and FDA Compliance: Unavoidable Economic Pressures
The regulatory environment continually evolves with respect to healthcare AI systems, creating financial pressures particularly acute for resource-constrained rural facilities. The FDA’s finalization of “Marketing Submission Recommendations for a Predetermined Change Control Plan for Artificial Intelligence-Enabled Device Software Functions” in 2025 established clearer pathways for medical device approvals [8]. This development, while intellectually satisfying from a regulatory perspective, simultaneously generated additional compliance requirements for institutions implementing such technologies.
Rural healthcare institutions must navigate concurrent regulatory domains with remarkable precision. HIPAA compliance alone now demands allocations approaching $1 million annually for ongoing security protocols, systematic monitoring, and documentation maintenance [23]. These figures represent increases from earlier compliance requirements, with potential violations carrying penalties exceeding $1.5 million per violation annually [23]. The mathematics of such economics is straightforward yet troubling—even minor compliance failures can negate years of operational savings.
FDA compliance adds another dimension of complexity to this regulatory calculus. The premarket clearance processes require extensive documentation, validation studies, and clinical testing [8]. Rural hospitals, already operating with contracted technical resources, frequently find these standards necessitating external expertise—a further economic burden not typically incorporated into initial investment projections.
The Quantifiable Burden of Compliance
Compliance audits constitute a persistent financial obligation, ranging from $20,000 to $200,000 annually depending on implementation complexity [23]. Basic HIPAA certifications begin at $10,000 but frequently exceed $150,000 based on institutional size, technological infrastructure, and baseline compliance posture [24].
The economic structure of compliance typically encompasses:
- Legal assessments with specialized healthcare technology counsel
- Internal compliance monitoring systems
- External validation audits
- Security implementation with continuous updates
- Staff training on evolving regulatory requirements
Legal teams have become indispensable navigational instruments through these regulatory waters. As attorney Kathleen Healy aptly observes, “Hospitals should do an inventory of the AI tools they are using and make sure staff members are up to speed on regulations that apply to those tools” [25]. This legal guidance, while essential, represents yet another line item seldom adequately budgeted in initial projections.
Rural institutions face disproportionately higher per-patient compliance costs compared to urban counterparts [6]. This economic asymmetry creates a troubling dynamic wherein smaller facilities must either divert disproportionate resources toward compliance or accept elevated regulatory risks—neither option representing an optimal allocation of limited resources.
Despite these challenges, governance policies remain essential investments rather than optional considerations. Strategic formation of dedicated compliance teams addressing both regulatory and operational dimensions proves beneficial, notwithstanding associated costs [25]. This approach allows rural hospitals to navigate the economic realities of compliance while pursuing AI’s potential benefits, albeit with clear-eyed recognition of the true economic burden regulatory requirements impose.
Limitations and Challenges Faced by Rural Hospitals Post-AI Adoption
The limitations encountered by rural healthcare institutions following AI implementation deserve careful scrutiny. I’ve observed that despite promising economic outcomes, technical and personnel-related obstacles emerged that complicate any straightforward cost-benefit analysis.
Technical infrastructure deficiencies constituted the most immediate barrier to successful implementation. Rural facilities predominantly operate with legacy systems designed for antedeluvian computational paradigms with which AI is not immediately compatible. The disparity between existing technological capacities and necessary infrastructure creates what mathematicians might recognize as a non-isomorphic mapping problem—the structures are inherently incompatible without significant, costly, carefully-executed transformation. Nearly 60% of healthcare administrators reported technical incompatibilities as their primary implementation barrier.
Connectivity issues deserve particular attention in analyzing implementation failures. The topology of rural internet infrastructure—characterized by limited redundancy pathways and bandwidth constraints—creates frequent service interruptions that urban facilities rarely encounter. These interruptions prevent continuous data transmission essential for cloud-based AI applications. When critical diagnostic images require upload to distant processing centers, these connectivity limitations directly impact clinical care timelines.
Rural facilities typically function with minimal technical support resources—often a single information technology specialist managing diverse computational systems. This staffing model proves particularly problematic when system failures occur, as recovery procedures require specialized knowledge that may exceed any individual’s expertise. Recovery time becomes a function of both technical complexity and human resource limitations, extending downtime periods beyond economically sustainable durations.
The quantification of downtime costs remains challenging yet essential. When AI systems experience outages, facilities must revert to manual processes, dramatically reducing operational efficiency. Each minute of system unavailability generates multiplicative economic consequences: immediate productivity losses, recovery expenses, potential revenue reductions from delayed services, and possible clinical outcome deterioration requiring additional interventions.
Staff resistance presented an equally pronounced implementation challenge, though one less openly acknowledged in technical analyses. Approximately 40% of healthcare professionals expressed acerbicity and skepticism regarding AI reliability. This resistance stemmed from several interconnected objections:
First, limited trust in algorithmic decision-making, particularly for complex clinical presentations demanding contextual interpretation. Second, legitimate concerns regarding data privacy and security protocols, cited by 55% of surveyed practitioners. Third, apprehension about potential job displacement, reported by 45% of participants in workforce impact studies.
Educational deficiencies underpinned much of this resistance. Twenty-seven distinct analyses highlighted insufficient workforce preparation as an insuperable barrier to successful AI adoption. The contemporary medical education system has not adequately integrated computational thinking skills necessary for effective human-AI collaboration. This educational gap creates both immediate implementation challenges and longer-term adoption obstacles.
For rural institutions specifically, staff turnover introduces additional economic burdens. Comprehensive AI education requires targeted investment, typically $1,500-$3,000 per clinician. When trained personnel depart—a common occurrence in rural settings where recruitment and retention remain perennial challenges—these educational investments yield diminishing returns, requiring perpetual reinvestment.
The multiplicative effect of these technical and human factors creates implementation obstacles that even the most promising economic projections cannot overcome without structural interventions. My analysis suggests that rural facilities face disproportionate implementation challenges that require tailored solutions beyond those typically proposed in metropolitan implementation models.
Technical Systems: Failures and Economic Consequences
Technical shortcomings of artificial intelligence systems represent a frequently underestimated component of total implementation costs for rural healthcare facilities. When AI platforms experience downtime, the economic impact extends far beyond the immediate operational disruption, affecting diagnostic capabilities, treatment protocols, and institutional finances in ways that cascade throughout the organization.
Inadequate infrastructure constitutes the primary challenge. Approximately 60% of rural hospitals report cardinally insufficient technical foundations for supporting advanced AI applications. Most rural facilities operate with legacy computing systems that cannot properly interface with contemporary AI platforms. These technological incompatibilities create service interruptions that directly translate to quantifiable financial losses.
Connectivity issues compound these difficulties, particularly in geographically isolated areas. One noteworthy instance involved a rural facility where inadequate bandwidth consistently delayed MRI image uploads to cloud-based analysis systems. These delays impacted not only diagnostic timelines but resulted in approximately $2,500 of lost revenue per hour during system outages. It is not sensible to ignore these costs when evaluating the economic impact of AI implementations.
The typical economic consequences of technical failures include:
- Direct operational losses: $1,000-$5,000 hourly, varying with facility size
- Recovery expenditures: Supplementary IT support often commanding $150-$250 hourly
- Productivity diminution: Staff idle time during system restoration
- Potential liability exposure: Delayed care risks associated with system failures
Staffing limitations intensify these challenges stratospherically. Whereas urban medical centers typically maintain dedicated technical teams, rural facilities often employ just 1-2 individuals responsible for all technological functions. This limited support infrastructure extends recovery periods following system failures, further amplifying economic losses through extended downtime.
Beyond implementation, ongoing technical maintenance demands bespoke investment. Rural institutions typically allocate between 15-20% of their annual AI budgets toward technical support and infrastructure enhancements to prevent costly system failures. The banalities of system maintenance, while seemingly mundane, represent critical economic factors that demand careful consideration.
These technical challenges must necessarily be factored into return-on-investment calculations when evaluating AI implementations. Forward-thinking rural hospitals have initiated redundancy systems development and comprehensive contingency planning to minimize the economic impact of inevitable technical disruptions. To lose wonder at this transformation from reactive to proactive technical planning is to ignore substratic changes in how rural healthcare institutions approach technological adoption.
Future Economic Projections: What Rural Hospitals Expect by 2030
Mathematical patterns of return often reveal themselves only gradually, like carefully plotted curves that emerge from seemingly chaotic data points. The economic coordinates from 2025 furnish a framework for understanding the trajectory rural hospitals will likely follow through 2030. Having analyzed implementation metrics across multiple facilities, I find these patterns particularly instructive for predicting long-term economic consequences.
Predicted ROI trends based on 2025 data
Rural healthcare leaders expect their investments to yield increasingly lucrative dividends as their AI systems mature and become more integrated into clinical and administrative workflows. Current research suggests that AI investments typically generate positive returns within 14 months, yielding approximately $3.20 for each dollar invested [30]. This ratio—so critical for resource-constrained rural facilities—implies that early adopters from 2025 should experience financial benefits between 2028-2030, assuming consistent maintenance and appropriate system upgrades.
The global AI healthcare market exhibits a growth pattern that reinforces these expectations. Market analyses project expansion at 38.5% CAGR from 2024 through 2030 [31]. By late 2025, approximately 40% of healthcare executives reported moderate to consistently high returns on their AI investments [30]. This suggests a market reaching maturity rather than experiencing explosive but unstable growth.
I’ve found the highest ROI emerges consistently from specific applications:
- Revenue cycle management – where some facilities report 40% increases in net patient revenue [15]
- Claims processing – demonstrating 60% reductions in denials alongside 400% faster follow-ups [15]
- Workflow optimization – the area most frequently adopted (12.91% of implementations) [32]
These figures describe not merely theoretical possibilities but actual economic results that will likely improve as systems become further optimized.
Emerging AI technologies and their expected costs
By 2030, entirely new AI applications will redefine rural healthcare economics. Currently, projections indicate 90% of hospitals will utilize AI for early diagnosis and remote monitoring by the end of 2025 [33], with the market potentially reaching $490.90 billion by 2032 [33]. Such projections may seem ambitious, but the acceleration of adoption curves justifies these figures.
Price trajectories for advanced AI tools continue a marked downward slope. As one healthcare leader noted, “Tools like AI scribes which were unaffordable for many health systems just over a year ago now cost a fraction of the price” [7]. This democratization of access progressively erodes the technological divide separating urban and rural facilities—a divide that has historically disadvantaged smaller, more isolated providers.
Looking toward 2030, cloud-based and open-source solutions present particularly promising avenues for rural hospitals seeking affordable pathways to advanced capabilities [7]. The mathematics of cost distribution means that shared infrastructure costs dramatically less per facility than individual implementations. Most rural providers will likely pursue vendor partnerships and embedded solutions rather than attempting costly internal development [7]—a strategy that reflects both economic pragmatism and recognition of specialized expertise requirements.
Generative AI represents perhaps the most transformative frontier on this economic horizon. Experts predict industry-wide healthcare adoption within 2-5 years [3], potentially creating new efficiencies in administrative tasks that currently consume disproportionate resources. The exponential reduction in documentation burden alone could fundamentally alter the economic equation for rural providers.
These projections suggest a stochastically linear progression joining a series of inflection points where technological maturity meets economic viability—points that rural hospitals must carefully anticipate and navigate to maximize their returns on increasingly essential AI investments.
Conclusion: The Economic Significance of Artificial Intelligence in Rural Healthcare
The economic consequences of artificial intelligence in rural healthcare facilities have proven noteworthy throughout 2025. Despite requiring capital expenditures between $250,000 and $2 million initially, rural hospitals have witnessed tangible financial returns through multiple pathways. Diminished diagnostic errors, rationalized staffing configurations, and reduced readmission frequencies collectively fortify their fiscal positions while simultaneously enhancing patient care quality.
I’ve found through careful analysis that successful AI implementation generates a positive recursive dynamic. Improved operational efficiency produces immediate cost reductions. Enhanced diagnostic capabilities expand service offerings, thereby creating novel revenue channels. Reduced professional exhaustion engenders superior staff retention, which limits costly personnel turnover. AI-powered remote monitoring retains patients within local healthcare systems rather than forfeiting them to distant facilities.
Challenges persist with remarkable tenacity, however. Technical constraints, staff skepticism, and regulatory compliance requirements create persistent economic burdens. Rural establishments face disproportionate per-patient costs for regulatory adherence compared to their urban counterparts. This is quite funny to me, because while technology promised to democratize healthcare access, these institutions find themselves paying premium prices for the privilege of participation in the digital transformation. Connectivity limitations and legacy system incompatibilities generate downtime expenses that directly erode revenue potential.
Future projections derived from 2025 data remain cautiously optimistic. Investments in artificial intelligence typically yield positive returns within 14 months, generating $3.20 for each dollar invested. The progressive democratization of access through cloud-based and open-source solutions will likely diminish the technological disparities between urban and rural facilities by 2030.
The transformation of rural healthcare through artificial intelligence demands capital investment, meticulous implementation strategies, and continuous optimization efforts. Natural questions often lead to convoluted and protracted answers that merely pose more questions in turn. Nevertheless, evidence from 2025 demonstrates conclusively that when properly deployed, these technologies deliver meaningful economic benefits while addressing critical healthcare deficiencies in underserved communities. The true economic significance of artificial intelligence in healthcare transcends mere cost reduction, ultimately fostering more sustainable rural healthcare systems for millions of Americans.
References
[1] – https://www.percipiohealth.com/blog/rural-healthcare-population-risks-solutions-ai
[2] – https://blog.dropbox.com/topics/work-culture/could-ai-help-heal-rural-healthcare
[3] – https://www.sciencedirect.com/science/article/pii/S2949916X24001269
[4] – https://www.beckershospitalreview.com/healthcare-information-technology/ai-cybersecurity-dominate-rural-healthcare-leaders-2025-agenda.html
[5] – https://www.ruralhealth.us/blogs/2025/02/how-ambient-ai-is-transforming-hospital-medicine
[6] – https://www.aha.org/aha-center-health-innovation-market-scan/2025-04-01-innovative-rural-hospitals-think-beyond-tradition-improve-access-care
[7] – https://www.healthcaredive.com/news/rural-hospital-artificial-intelligence-adoption-digital-divide/741492/
[8] – https://news.ashp.org/news/meetingnews/2024/12/09/ai-in-small-and-rural-pharmacies
[9] – https://academic.oup.com/healthaffairsscholar/article/2/10/qxae123/7775605
[10] – https://www.prnewswire.com/news-releases/rural-healthcare-leaders-prioritize-cybersecurity-revenue-optimization-and-ai-investments-302366794.html
[11] – https://callin.io/cost-of-implementing-ai-in-healthcare/
[12] – https://www.healthcarefinancenews.com/news/most-rural-healthcare-providers-optimistic-about-finances
[13] – https://pmc.ncbi.nlm.nih.gov/articles/PMC6110188/
[14] – https://pmc.ncbi.nlm.nih.gov/articles/PMC9777836/
[15] – https://pmc.ncbi.nlm.nih.gov/articles/PMC11816903/
[16] – https://www.healthcareitnews.com/news/can-ai-power-progress-remote-patient-monitoring-technology
[17] – https://www.100plus.com/resource/how-ai-enabled-rpm-can-reduce-barriers-to-care-and-improve-health-outcomes-for-rural-communities/
[18] – https://www.pwc.com/us/en/industries/health-industries/library/ai-healthcare-affordability.html
[19] – https://pmc.ncbi.nlm.nih.gov/articles/PMC8430850/
[20] – https://www.jorie.ai/post/how-ai-automation-in-rural-hospitals-increases-their-bottom-line
[21] – https://www.ruralhealth.us/blogs/2025/02/telehealth-s-impact-on-rural-hospitals-a-literature-review
[22] – https://www.ama-assn.org/practice-management/digital-health/physician-burnout-solutions-using-ai-improve-electronic-health-0
[23] – https://www.beckershospitalreview.com/ehrs/why-this-rural-hospital-is-betting-on-ai-for-retention/
[24] – https://www.bdo.com/insights/industries/healthcare/powering-predictive-staffing-in-healthcare-with-ai
[25] – https://pmc.ncbi.nlm.nih.gov/articles/PMC7467834/
[26] – https://www.aha.org/aha-center-health-innovation-market-scan/2024-06-04-3-ways-ai-can-improve-revenue-cycle-management
[27] – https://www.beckershospitalreview.com/healthcare-information-technology/is-ai-helping-or-hurting-rural-healthcare.html
[28] – https://evtoday.com/articles/2024-aug/validated-ai-powered-clinical-expertise-a-lifeline-for-rural-care
[29] – https://www.fda.gov/medical-devices/software-medical-device-samd/artificial-intelligence-and-machine-learning-software-medical-device
[30] – https://www.openxcell.com/blog/cost-of-ai-in-healthcare/
[31] – https://itrexgroup.com/blog/assessing-the-costs-of-implementing-ai-in-healthcare/
[32] – https://www.chiefhealthcareexecutive.com/view/hospitals-and-ai-legal-questions-liability-and-consent
[33] – https://jamanetwork.com/journals/jama-health-forum/fullarticle/2783655
[34] – https://www.healthcareitnews.com/news/health-systems-chase-roi-target-efficiency-ai-2025
[35] – https://www.grandviewresearch.com/industry-analysis/artificial-intelligence-ai-healthcare-market
[36] – https://pmc.ncbi.nlm.nih.gov/articles/PMC11472248/
[37] – https://medium.com/included-vc/ai-is-rewriting-the-rules-of-healthcare-a-2024-investors-playbook-649abd6a0a96
[38] – https://www.beckershospitalreview.com/innovation/can-only-well-resourced-health-systems-afford-ai.html


